


Giorgia Paglia1, Silvano Gallus2 , Rolando Crippa1, Giovanni Evangelista Mancini3, Piergiorgio Zuccaro4, Luigi Paglia1
1Fondazione Istituto Stomatologico Italiano (ISI), Milano
2Dipartimento di Epidemiologia; IRCCS - Istituto di Ricerche Farmacologiche “Mario Negri”, Milano
3Fondazione ANDI Onlus
4Consulente Scientifico del progetto No Smoking Be Happy - Fondazione Umberto Veronesi
In tempi di crisi economica e di spending rewiew ci si rende sempre più conto di come puntare sulla prevenzione sia il miglior investimento possibile. Anche noi dentisti dobbiamo prestare sempre più attenzione alle tematiche preventive del cavo orale: un’opportunità per ridare slancio e credibilità a tutta la nostra attività e categoria. Il dentista potrebbe infatti diventare un elemento fondamentale per la promozione di corretti stili di vita, data la stretta relazione che lo lega ai suoi pazienti, la possibilità, che gli è peculiare, di seguirli con costanza nel tempo e la stima di cui gode. Pertanto, uno studio inglese ha recentemente mostrato come i genitori di bambini accettassero di buon grado che i dentisti pediatrici proponessero a genitori e figli informazioni sull’educazione preventiva e informazioni sulla cessazione del fumo durante le visite private (Davidson et al., 2013).
Quando si parla di tematiche preventive in generale, e in particolare di prevenzione del cavo orale, viene subito in mente il fumo di tabacco, la principale causa evitabile di mortalità e di incidenza di malattie croniche. Nonostante la tendenza favorevole degli ultimi decenni della prevalenza di fumatori in Italia (Gallus et al., 2013A), ogni anno nel nostro Paese il fumo è ancora responsabile di più di 70.000 morti (Gallus et al., 2011). Di questi decessi, più di 1500 avvengono a causa del tumore del cavo orale e faringe (Gallus et al., 2011). È chiaro quindi che il fumo rimane la prima causa di morte per malattia delle alte vie respiratorie. Non solo, il fumo esercita il suo effetto negativo anche sull’esito di molteplici cure odontoiatriche. Pertanto, nelle terapie implantari e parodontali il fumo espone a un maggior rischio di insuccessi terapeutici (Johnson et al., 2001; Johnson et al., 2004); inoltre, il fumo genera pigmentazioni dentarie che rendono meno efficaci le tecniche di sbiancamento oggi tanto richieste. Analogamente, affrontare il problema dell’alitosi significa migliorare “l’estetica“ del respiro poiché il fumatore ha un alito cattivo rispetto al non fumatore, e rientra fra i compiti dell’odontoiatra/igienista affrontare anche questo tipo di problemi.
Un altro esempio è quello della smoker face (Okada et al., 2013): proprio in un periodo in cui ci affanniamo a migliorare l’aspetto estetico del paziente non ha senso non combattere contro il “killer” maggiore del sottocutaneo: il fumo, con la vasocostrizione e i prodotti tossici che produce (Paglia et al., 2013). Le stesse problematiche si possono riscontrare quando si parla di alimentazione. Per esempio la baby bottle syndrome, i cui effetti nefasti riscontriamo quotidianamente nei nostri pazienti, è causata principalmente da una scorretta educazione alimentare (Chankaka et al., 2012). Rendere lo studio odontoiatrico un polo di orientamento nella lotta contro il fumo e nella promozione di corretti stili di vita risulta un progresso importante per conquistare e offrire ai propri pazienti un maggiore benessere complessivo. Il primo passo di questa strategia non può che essere la raccolta di informazioni su come si comporta e su quello che pensa a questo proposito il dentista. Vista la carenza di informazioni presenti in letteratura sulla salute generale dei dentisti (Puriene et al., 2007), è di fondamentale importanza capire pertanto se lo stesso dentista segua stili di vita adeguati per potere dare il buon esempio, cosa faccia e cosa sia disposto a fare per se stesso e per i propri pazienti. Abbiamo pertanto condotto su questo tema un’indagine supportata dall’editore Tecniche Nuove, da Fondazione ISI (Istituto Stomatologico Italiano, Milano), da Fondazione ANDI Onlus e da Fondazione Veronesi all’interno del progetto “No Smoking Be Happy - Per il tuo sorriso”.
Materiali e metodi
Per valutare l’atteggiamento del dentista italiano rispetto agli stili di vita e la sua propensione a occuparsi di questo tema abbiamo messo a punto un questionario da compilare on-line con 11 domande (Allegato 1). Nell’aprile 2014 il questionario è stato inviato via e-mail a un indirizzario di 24.562 dentisti italiani. Di questi, 4692 (il 19,1%) hanno ricevuto e letto la mail, e 1048 (il 4,3%) hanno seguito il link al questionario.
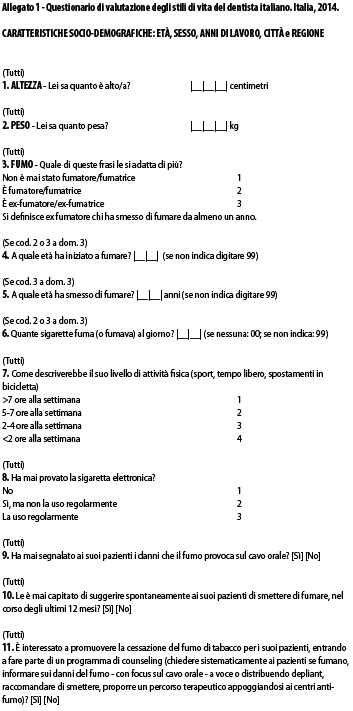
L’indagine - rimasta disponibile on-line per la compilazione per una settimana - oltre alla raccolta di dati socio-demografici, richiedeva il peso e l’altezza dell’intervistato per poter ricavare l’indice di massa corporea (IMC: kg/m2); nelle successive 4 domande venivano indagate le abitudini rispetto al fumo e all’utilizzo della sigaretta elettronica. Venivano poi approfonditi il livello di attività fisica nel tempo libero e la propensione a comunicare ai pazienti i danni che il fumo causa al cavo orale. Da ultimo, veniva richiesta la disponibilità a promuovere la cessazione del fumo ai propri pazienti. Le differenze per sesso e stato di fumo della distribuzione percentuale di svariate caratteristiche individuali sono state analizzate tramite il test chi-quadrato.
Risultati
Nell’arco di una settimana 1048 dei dentisti ai quali è stato indirizzato l’invito a partecipare all’indagine hanno seguito il link al questionario on-line e, di questi, 883 (84,3%) hanno fornito almeno una informazione sugli stili di vita e sono pertanto stati analizzati.
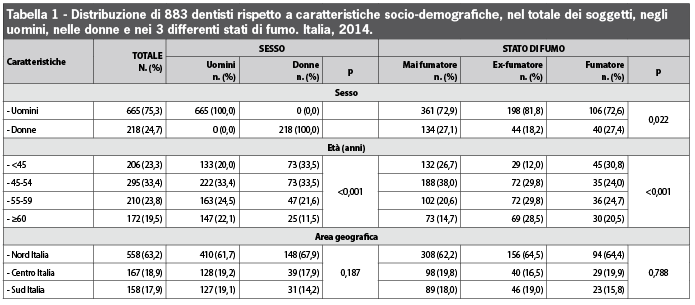
La Tabella 1 mostra la distribuzione dei dentisti Italiani per caratteristiche socio-demografiche nel totale dei soggetti, nei maschi e nelle femmine e separatamente nei mai fumatori, negli ex-fumatori e nei fumatori. L’età media di chi ha risposto era di 51 anni e la media degli anni di esercizio professionale del campione era di 29 anni. Il 25% dei casi era di sesso femminile e il 75% maschile. Il 63% del campione risiedeva in Nord Italia, il 19% in Centro e il 18% al Sud. La distribuzione per età era differente tra i sessi (p<0,001) e tra i tre stati di fumo (p<0,001). Le donne erano meno frequentemente ex-fumatrici rispetto agli uomini e più frequentemente fumatrici o mai fumatrici (p=0,022). Non si apprezzavano invece differenze statisticamente significative per area geografica tra i sessi e i differenti stati di fumo.
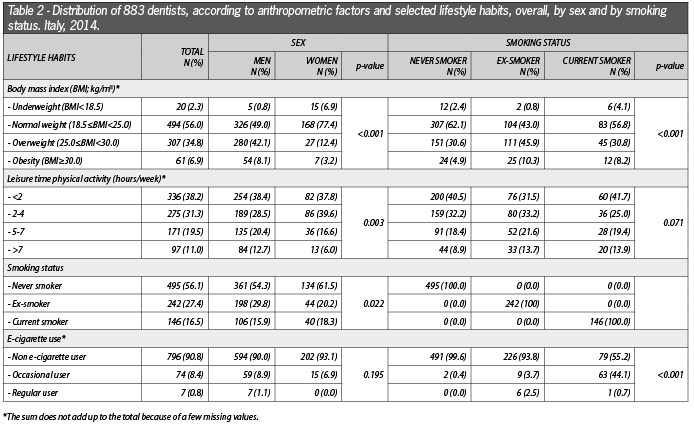
Il peso medio del campione era di 75 kg per un’altezza media di 175 cm. Il 2% del campione era sottopeso (1% degli uomini e 7% delle donne), il 56% era normopeso (49% degli uomini e 77% delle donne), il 35% sovrappeso (42% degli uomini e 12% delle donne) e il 7% obeso (8% degli uomini e 3% delle donne) (Tabella 2).
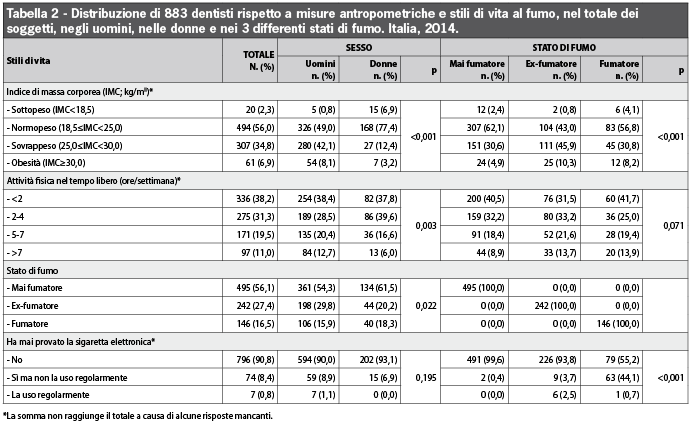
L’IMC era statisticamente più alto tra gli uomini rispetto alle donne (p<0,001) e negli ex-fumatori rispetto ai mai fumatori o ai fumatori attuali (p<0,001). Pertanto, l’obesità era più frequente tra gli ex-fumatori (10%) e tra i fumatori (8%) rispetto ai non fumatori (5%). Il 38% del campione praticava attività fisica nel tempo libero per meno di due ore a settimana, il 31% tra 2 e 4 ore, il 20% tra 5 e 7 ore e l’11% per più di 7 ore a settimana. Gli uomini facevano attività fisica più frequentemente rispetto alle donne (p = 0,003). Pertanto, il 13% degli uomini, ma solo il 6% delle donne, praticavano attività fisica per più di 7 ore a settimana. Il 56% del campione non aveva mai fumato (54% degli uomini e 62% delle donne), il 17% era un fumatore (16% degli uomini e 18% delle donne) e il 27% era un ex fumatore (30% degli uomini e 20% delle donne). L’età media di inizio dell’abitudine al fumo è di 18 anni. Il 91% del campione non aveva mai provato la sigaretta elettronica, l’8% l’aveva provata, mentre l’1% del campione la usava regolarmente. Tra i fumatori, il 45% l’aveva provata e l’1% la usava regolarmente, mentre tra gli ex-fumatori il 4% l’aveva provata e il 3% la usava regolarmente. Il 98% del campione riportava di aver segnalato i danni che il fumo provoca al cavo orale (Tabella 3).
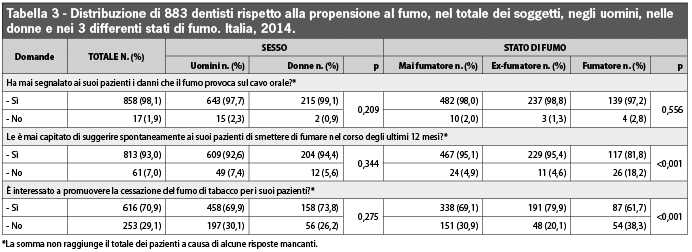
Non si riscontravano differenze significative per sesso e stato di fumo. Il 93% del campione (95% dei non fumatori e 82% dei fumatori; p<0,001) riportava di aver suggerito ai propri pazienti di smettere di fumare negli ultimi 12 mesi. Il 71% del campione era interessato a promuovere la cessazione del fumo di tabacco nei propri pazienti dichiarandosi disponibile a entrare a far parte di un programma strutturato di counseling antifumo. I dentisti interessati erano più frequentemente gli ex-fumatori (80%), e coloro che non avevano mai fumato (69%) rispetto ai fumatori attuali (62%).
Discussione
Hanno risposto al questionario colleghi con alle spalle un’attività professionale di circa 30 anni e un’età media di 50 anni. Solo il 23 % del campione è sotto i 45 anni di età. Nel totale del campione, 3 su 4 partecipanti sono uomini e solo 1 su 4 è donna. Tuttavia, se tra gli anziani (età >60 anni) le donne sono solo il 15%, tra i giovani (età <45 anni) le donne crescono al 35%. Questo dato conferma che, pur rimanendo preponderanti gli uomini in ogni fascia di età, anche l’Odontoiatria, come peraltro la Medicina, nelle giovani leve si tinge sempre più di rosa.
Il Nord Italia con il 63% delle risposte totali al questionario è la macro regione italiana che si è mostrata più sensibile alla tematica distanziando di parecchie misure sia il Centro (18%) che il Sud Italia (18%). La distribuzione del campione è comparabile con quella del totale degli invitati a partecipare all’indagine (58% in Nord Italia, 23% in Centro e 20% al Sud). L’eccesso di risposte dal Nord Italia può essere spiegato dal maggior tasso di fidelizzazione presente in quell’area tra i lettori della rivista Il Dentista Moderno che ha materialmente veicolato il questionario. Il 42% del campione risultava in sovrappeso od obeso e il 7% obeso. Queste stime sono in linea con quelle riscontrate nel totale della popolazione adulta italiana (42% sovrappeso/obeso e 9% obeso) secondo un’indagine Doxa condotta nel 2010 (Gallus et al., 2013C), e leggermente inferiore a quelle relative agli adulti italiani di mezza età (45-64 anni), dove il 51% risultava in sovrappeso od obeso e l’11% obeso. Le differenze in termini di obesità tra uomini e donne possono essere spiegate, almeno in parte, dalla più giovane età delle donne in questo campione. Tra gli ex fumatori, il sovrappeso/obesità sale al 56% e l’obesità al 10%. Queste stime, seppur non aggiustate per potenziali fattori confondenti, inclusa l’età, confermano la nota tendenza a ingrassare tra gli ex-fumatori (Gallus et al., 2013C) e l’importanza di applicare norme di igiene alimentare atte a controllare il peso corporeo in chi decide di smettere di fumare. Globalmente l’attività fisica è per il 38% del campione sotto le 2 ore a settimana e per quasi il 70% sotto le 4 ore a settimana. Queste stime confermano i risultati di altri studi condotti altrove che mostravano come la professione del dentista sia generalmente associata a un limitato livello di attività fisica (Ashim, Al-Ali, 2013; Puriene et al., 2007).
Il 17% del campione totale si dichiara fumatore. Questa stima è inferiore rispetto alla media nazionale, che si attesta intorno al 21% secondo un’indagine rappresentativa della popolazione adulta italiana e condotta da Doxa nel 2012 (Gallus et al., 2013A). La prevalenza di fumo tra i dentisti maschi (16%) è sostanzialmente inferiore rispetto alla media dei maschi adulti italiani (25%). Al contrario, la prevalenza di fumatrici tra le dentiste femmine (18%) supera addirittura la media delle donne italiane (17%; Gallus et al., 2013A). Se pensiamo che tra il personale sanitario - compreso quello odontoiatrico - è lecito attendersi un maggior grado di sotto-riporto dell’abitudine al fumo, dovuto a una alta pressione sociale verso la cessazione del fumo (Rebagliato, 2002), questi risultati sono deludenti e arrivano a essere letti come sconfortanti, specialmente se confrontati con le ridottissime prevalenze di fumo osservate tra i dentisti degli Stati Uniti (3%; Sarna et al., 2010) e tra gli studenti dell’ultimo anno di Odontoiatria in Australia (5%; Messer, Calache, 2012). I risultati sulla sigaretta elettronica non sorprendono, essendo in linea con quelli osservati nella popolazione generale italiana (Gallus et al., 2014). Molto al di là delle aspettative appaiono invece i risultati relativi agli ultimi tre quesiti. Praticamente la totalità dei dentisti che ha partecipato a questa indagine (il 98% del campione) dichiara di aver segnalato almeno una volta i danni che il fumo provoca al cavo orale nei propri pazienti. Il 93% ha recentemente messo in atto veloci pratiche volontarie di minimal advice antifumo.
Scende però al 71% la proporzione dei clinici interessati nel mettere in atto pratiche più strutturate di promozione della cessazione dell’abitudine al fumo. Sembrerebbe quindi che la gran parte dei dentisti sia favorevole a spiegare al paziente le conseguenze della dipendenza dal fumo sottolineando le correlazioni che questa abitudine ha con la salute del cavo orale, ma meno interessata ad attuare nella propria realtà ambulatoriale percorsi di disassuefazione. Comunque, il fatto che più di 2 dentisti italiani su 3 siano interessati a promuovere la cessazione del fumo di tabacco per i propri pazienti è un’ottima notizia che potrebbe avere notevoli implicazioni da un punto di vista di controllo del tabagismo e di salute pubblica. Gli operatori sanitari giocano infatti un ruolo chiave nella prevenzione dal fumo di tabacco, in quanto sono considerati come modello dai pazienti (Ferketich et al., 2008).
La figura professionale che meglio può promuovere la salute a livello individuale è sempre stata considerata quella del medico di famiglia. Ciononostante, alcune indagini hanno dimostrato come soltanto pochi medici di famiglia in Italia promuovano corretti stili di vita e suggeriscano ai fumatori di smettere di fumare (Ferketich et al., 2008; Gallus et al., 2013B). Ne consegue che, durante le visite con i pazienti, il dentista ha la possibilità di diventare, tra i vari operatori sanitari, il principale promotore di corretti stili di vita. Inoltre, egli ha verosimilmente una posizione addirittura privilegiata rispetto al medico di famiglia, dal momento che i giovani in salute, coloro pertanto che maggiormente otterrebbero un beneficio, vengono a contatto più frequentemente con i dentisti rispetto al proprio medico di base. È anche per questo che c’è sempre maggiore interesse nel chiedere ai dentisti di promuovere la cessazione del fumo di tabacco durante le loro visite private (Carr et al., 2012; Gonzales, 2014). Ciononostante è necessario fornire un adeguato training ai dentisti che vogliono promuovere il controllo del tabagismo tra i propri pazienti, dal momento che anche tra i professionisti degli Stati Uniti sono state riscontrate alcune lacune di preparazione (Prakash et al., 2013). Per ora, inoltre, le visite dentistiche rimangono un’opportunità sotto-utilizzata per il trattamento della dipendenza del tabacco (Shelley et al., 2012). La limitazione maggiore dello studio riguarda il relativamente basso tasso di risposta (3,6%) dei dentisti invitati a partecipare alla presente indagine che non consente di garantire la rappresentatività del campione rispetto alla totalità dei dentisti Italiani. Ciononostante, i partecipanti hanno una distribuzione comparabile per area geografica rispetto alla totalità di coloro ai quali è stato mandato l’invito a partecipare. Inoltre, la distribuzione per sesso e la media di età riflette la realtà dei dentisti italiani. Infine, gli 883 partecipanti rappresentano una proporzione non trascurabile (circa il 2%) di tutti i dentisti italiani.
Conclusioni
Il campione da noi esaminato, sebbene non rappresentativo della popolazione odontoiatrica italiana, può essere utile per alcune importante riflessioni. Sembra esistere un importante interesse all’interno della categoria rispetto alla promozione di corretti stili di vita. In particolare, il sottogruppo degli odontoiatri ex-fumatori si è dimostrato particolarmente attivo e propositivo sia nell’informare i propri pazienti sui danni provocati dal fumo (99%) sia nel mettere in pratica azioni di minimal advice antifumo (95%) e sarebbe pronto, dopo adeguata formazione, ad attivare nel proprio ambulatorio percorsi di disassuefazione sistematica (80%). Il problema sta in quel 17% di dentisti, prevalentemente femmine, che ancora mantiene il vizio del fumo e che meno frequentemente (o meno efficacemente) ne promuove la cessazione tra i suoi pazienti. Il primo obiettivo da raggiungere è pertanto quello di fare smettere di fumare l’intera categoria degli odontoiatri italiani al più presto. Del resto, come il dentista si rende subito conto se un paziente fuma o meno, è vero anche il contrario. Per rispetto nei confronti dei pazienti tutti, ma soprattutto dei non fumatori, il dentista dovrebbe astenersi dal fumare (almeno durante le ore lavorative). Una volta ridotta la prevalenza di fumatori tra i dentisti italiani a quella osservata negli USA o in Australia (<5%), vi sarà la grandissima opportunità di individuare gli operatori desiderosi di promuovere la cessazione tra i propri pazienti, in modo da fornire ai dentisti un’adeguata formazione. Verrà creata così una task force di operatori volontari in grado di ridurre sensibilmente il fumo in Italia, così da contribuire sostanzialmente a un miglioramento dell’attesa e della qualità di vita dei pazienti dei dentisti italiani, e quindi dell’intera popolazione del nostro Paese.
In this period of economic crisis and spending review, people realize that the best investment should rely on prevention. As dentists, we must pay more and more attention to prevention for the oral cavity: this may represent an opportunity to give back impulse and reliability to our activity and category. As a matter of fact, the dentists could become key characters, able to promote correct lifestyle habits for several reasons, including the close relationship with their patients, the unique opportunity to follow them constantly for long periods and the high reputation they are granted. For this reason a study conducted in UK has recently shown how children’s parents favourably accepted that pediatric dentists gave to them advices on smoking cessation, and to their children counseling on tobacco use during private practice (Davidson et al., 2013). When we talk about prevention for oral cavity, we immediately think about tobacco smoking, the main avoidable cause of death and chronic diseases. Despite the positive trend over the last few decades in Italy (Gallus et al., 2013A), every year tobacco smoking is responsible for more than 70.000 deaths (Gallus et al., 2011). Among those smoking attributable deaths, more than 1.500 are due to the cancers of the oral cavity and pharynx (Gallus et al., 2011). Tobacco smoking is therefore the first cause of mortality for mouth diseases. It also acts unfavourably on several dental treatments. In fact, smoking increases the risk of failures in implant and periodontal therapies (Johnson et al., 2001; Johnson et al., 2004); it also creates pigmentations on teeth which reduce the efficacy of whitening treatments, so popular today; tobacco smoking affects the breath as well: a smoker has likely a bad breath as compared to a non-smoker and it is one of the dentist’s or hygienist’s duty to face this kind of problems. Moreover, tobacco smoking has an unfavourable impact on facial aging (Okada et al., 2013): today that we continue to make attempts to improve the patients’ appearance, it is worthwhile to fight against the worst enemy of subcutaneous, i.e.: vasoconstriction and toxic effects caused by tobacco smoking (Paglia et al., 2013). Diet is also important when talking about prevention for the oral cavity. Thus, for example, the Baby Bottle Syndrome, whose negative effects are frequently observed in our patients, is caused by unfavourable dietary habits (Chankaka et al., 2012). Turning the dental office into an orienteering centre to fight against tobacco smoking and to promote correct lifestyle habits may be an important opportunity to offer the patients an effective improvement in their well-being. Since there is little information on the general health condition of the dentists (Puriene et al., 2007), it is very important to understand if the dentists themselves follow a correct lifestyle, if they may be good examples for their patients, and what they do or are ready to do for themselves and for their patients. With this aim, a survey has been conducted with the support of the publisher Tecniche Nuove, Fondazione ISI (Istituto Stomatologico Italiano – Milan), Fondazione ANDI Onlus and Fondazione Veronesi, within the project “No Smoking Be Happy – Per il tuo sorriso”. Material and methods Selected questions investigated habits connected to tobacco smoking and the use of the electronic cigarette. Moreover, other questions provided information on leisure time physical activity and the attitude to inform the patients on the harmful effects of smoking on oral cavity. Finally the availability for providing to smoking patients advices for smoking cessation was investigated. The differences between sexes and across strata of smoking status in the percent distribution of various lifestyle habits were analyzed using chi-square test. Results Table 1 shows the distribution of the Italian dentists according to their socio-demographic characteristics, overall, by sex and by smoking status. The average age was 51 years and the average duration of profession was 29 years. Overall, 25% were women and 75% men; 63% of the sample lived in northern Italy, 19% in central and 18% in southern Italy. The distribution by age was different according to sex (p <0.001) and according to smoking status (p<0.001). Women were less frequently ex-smokers than men and more frequently smokers or never-smokers (p=0.022). Geographic area did not significantly differ according to sex and smoking status. The average weight survey partecipants was 75 kg and the average height was 175 cm. Overall, 2% were underweight (1% of men and 7% of women), 56% had a normal weight (49% of men and 77% of women), 35% were overweight (42% of men and 12% of women) and 7% obese (8% of men and 3% of women) (Table 2). BMI was significantly higher in men than in women (p <0.001) and in ex-smokers than in never-smokers or in current smokers (p <0.001). Thus, obesity was more frequent among ex-smokers (10%) and current smokers (8%) than among non smokers (5%). Overall, 38% practiced leisure time physical activity less than 2 hours/week, 31% between 2 and 4 hours, 20% between 5 and 7 hours and 11% more than 7 hours/week. Men practiced physical activity more frequently than women (p = 0.003). Thus, 13% of men and only 6% of women practiced sport for more than 7 hours/week. Overall, 56% of dentists reported to be never smokers (54% of men and 62% of women), 17% current smokers (16% of men and 18% of women) and 27% ex-smokers (30% of men and 20% of women). The average age at starting smoking was 18 years. Of the entire sample, 91% never tried the electronic cigarette, 8% had tried it while 1% regularly used it. Among current (cigarette) smokers, 45% tried the e-cigarette and 1% regularly used it, while among ex-smokers 4% tried it and 3% regularly used it. Practically all the dentists (98%) reported to have informed their patients (at least once) on the harmful effects of smoking on the oral cavity (Table 3). No differences were found according to sex or smoking status. More than 93% of dentists (95% of non-smokers and 82% of smokers; p<0.001) reported that they suggested their smoking patients to stop smoking, at least once over the last 12 months. Overall, 71% of Italian dentists were interested in promoting smoking cessation among their patients and declared to be available to join a structured counselling programme against smoking. The dentists who were more interested into the topic were more frequently ex-smokers (80%), followed by never (69%) and current smokers (62%). Discussion Overall, 42% of participants were overweight or obese and 7% obese. These estimates are in broad agreement with those found for the overall adult Italian population (42% overweight/obese and 9% obese), observed in a survey conducted by DOXA in 2010 (Gallus et al., 2013C), and lower than those observed for middle aged Italians (45-64 years), among which 51% were overweight or obese and 11% obese. The difference concerning obesity between men and women can be explained, at least partially, by the young age of the women in this sample. Among ex-smokers, the prevalence of overweight/obese increased to 56% and obesity to 10%. These estimates, although not adequately adjusted for several confounding factors, confirm the tendency of ex-smokers to gain weight after smoking cessation (Gallus et al., 2013C), and show how important is to follow a correct diet in order to control the weight for those people who want to stop smoking. Almost 20% of the whole sample reported to be a current smoker. This prevalence is below the national adult smoking prevalence, which is 21% according to a survey conducted by DOXA in 2012 (Gallus et al., 2013A). The predominance of smokers among male dentists (16%) is lower than the average of Italian male adults (25%). The answers to the last three questions are beyond expectations. Practically all the dentists who took part to this survey (98% of the sample) reported to have informed at least once their patients about the harmful effects of tobacco smoking on oral cavity. Moreover, 93% have recently put into practice some voluntary minimal advice procedures against smoking. A lower proportion of dentists (71%) is interested in offering more structured practices to promote smoking cessation. It seems therefore that the large majority of dentists is favourable to advise their patients on the consequences of smoking addiction, underlining the association between this habit and the risk of cancer and other diseases of the oral cavity. In the meanwhile, they seem to be less prone to start specific counseling programmes in private practice. The general practitioner (GP) has always been considered the healthcare professional who may more effectively promote prevention at an individual level. Nevertheless some surveys have shown that just a limited proportion of GPs recommends smoking cessation to their smoking patients (Ferketich et al., 2008; Gallus et al., 2013B). Therefore, the dentist can become one of the main (if not the main) promoter of correct lifestyle habits, during the visits with their patients. In addition, as compared to GPs, dentists may take advantage of the fact that they more frequently visit young healthy people, which are those who benefit most from advices about correct lifestyles. Accordingly, the interest in identifying the dentist as a promoter for smoking cessation in private practice is rising (Carr et al., 2012; Gonzales, 2014). Nevertheless, it is important to offer an appropriate training to the dentists who want to promote smoking cessation among their patients. In the USA, for example, a lack of preparation on how to advise smokers to quit was observed among dentists (Prakash et al., 2013). At the moment, the visits at the dentist’s are still uexploited opportunity to treat the tobacco addiction (Shelley et al., 2012). The main limitation of this study is the low number of respondents (3.6%) with respect to the number of dentists invited to take part to the survey. This does not allow us to consider this sample representative of all the Italian dentists. However, from a geographical point of view, the number of participants is comparable to the total of dentists who were invited to the survey. Also the distributions according to sex and age reflect those of the overall population of Italian dentists. Finally, the 883 participants represent a non-negligible proportion (about 2%) of all the Italian dentists. Conclusions
In order to evaluate the attitude of the Italian dentists concerning lifestyles and their interest in this topic, we prepared an on-line questionnaire composed of 11 questions (Attachment 1). In April 2014 an invitation to partecipate was sent by e-mail to a mailing list of 24.562 Italian dentists. Among them, 4.692 (19.1%) received and read the e-mail and 1.048 (4.3%) followed the link to the on-line questionnaire. The questionnaire has been available on-line for one week. Besides socio-demographic information, self-reported data on weight and height was collected. Those data were used to derive participants’ body mass index (BMI: kg/m2).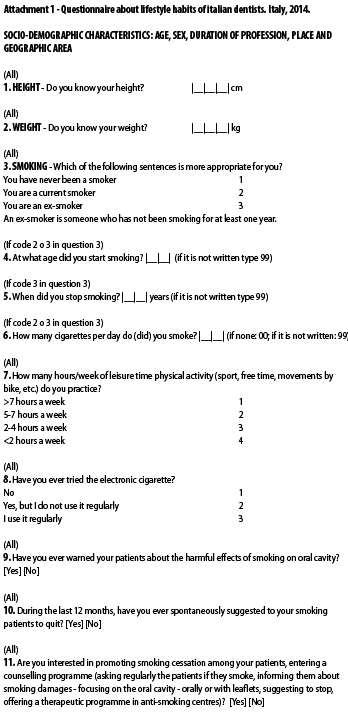
During one week 1048 dentists who were sent the invitation to take part in the survey, followed the link to the on-line questionnaire. Among them, 883 (84.3%) provided valid information on various lifestyle habits, and were therefore included in the analysis.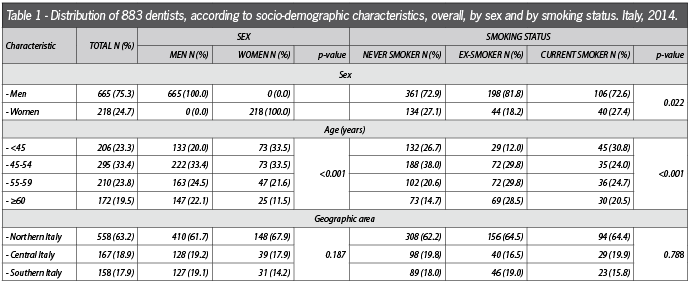

Survey participants are dentists who have been working for 30 years and with an average age of 50 years. Only 23% of participants are younger than 45. Considering the whole sample, 3 out of 4 participants are men. Among dentists aged >60 years, women are only 15%, whereas among younger dentists (age <45 years) women are 35%. This confirms that, although men are more frequent than women in every age group, there are more young female dentists than ever before. The same phenomenon is apparent among physicians. Northern Italy, with 63% of questionnaires, is the Italian area which resulted more interested in the topic, outdistancing significantly both central (18%) and southern Italy (18%). The distribution of the sample is however comparable to the total number of dentists invited to answer the questionnaire (58% in the North of Italy, 23% in the Centre and 20% in the South). The bigger amount of answers from the North of Italy can be explained by a higher grade of loyalty to the magazine Il Dentista Moderno, which spread the survey.
Less than 2 hours/week of physical activity was observed for 38% of the sample, and less than 4 hours/week for almost 70%. These data confirm the results of other studies, showing how the profession of the dentist is generally associated with a limited physical activity (Ashim, Al-Ali, 2013; Puriene et al., 2007).
On the contrary the amount of female smokers among dentists (18%) is higher than the average of Italian women (17%; Gallus et al., 2013A). We should take into account that smoking prevalence for dentists, as well as for other healthcare providers, is likely under-estimated, for the high social pressure to stop smoking (Rebagliato, 2002). More importantly, our results are quite disappointing and almost discouraging if we compare them to the smoking prevalence estimates among dentists from the USA (3%; Sarna et al., 2010) and among the students of the last year of dentistry from Australia (5%; Messer, Calache, 2012).
Findings on the electronic cigarette are in broad agreement with what has been recently observed among the Italian adult population (Gallus et al., 2014).
Anyway, the good news is that 2 out of 3 Italian dentists are interested in promoting smoking cessation to their patients. This may have important implications from a public health perspective. Healthcare providers play in fact an important role in tobacco control, because they are considered as models by their patients (Ferketich et al., 2008).
Even though it is not representative of the Italian dentists, this survey is useful for several aspects. Italian dentists appear to be extremely interested in promoting correct lifestyle habits to their patients. In particular, ex-smokers appeared active and purposeful in informing their patients about smoking damages (99%) and putting into practice minimal advice actions against smoking (95%). They would be ready, after a proper training, to start specific programmes for smoking cessation in private practice (80%). The problem lies in those 17% of dentists, mainly women, who still smoke and less frequently (or less effectively) promote smoking cessation.
The first step is therefore to make the whole category of Italian dentists smoke-free as soon as possible. Like a dentist immediately understands if a patient smokes, the other way round is true as well. The dentist should not smoke (at least during working hours) to respect their patients and in particular the non-smoking ones. When the amount of smokers among dentist is reduced to the same amount observed in the USA or in Australia (less than 5%), it will be easy to identify those professionals who are eager to promote smoking cessation among their patients, in order to offer a proper training. In this way a task force of volunteers will be created to reduce the diffusion of smoking in Italy, and contribute to an improvement of quality and expectancy of life.






{kind=link}
[…] [Fonte: Il dentista moderno] […]