

P. Maló1, C. Vidal2, C. Almeida2, I. Festas2, J. Nunes2, M. De Araújo Nobre3
1DDS, PhD, Oral Surgery Department; Maló Clinic Lisbon, Portugal
2DDS, Prosthodontic Department; Maló Clinic Lisbon, Portugal
3RDH, MSc Epi, Research and Development Department; Maló Clinic Lisbon, Portugal


Case description
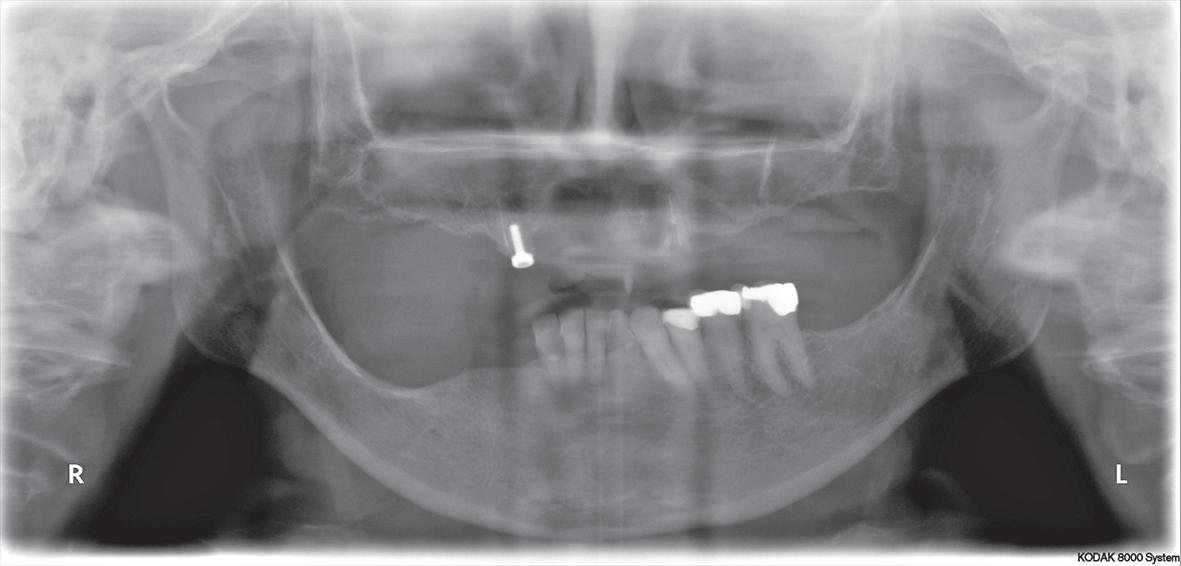
Female patient, aged 65, attended the private practice (Maló Clinic Lisbon, Portugal) complaining about her present rehabilitation with removable prostheses associated with diminished masticatory capability and esthetic appearance. Her main goal was to obtain
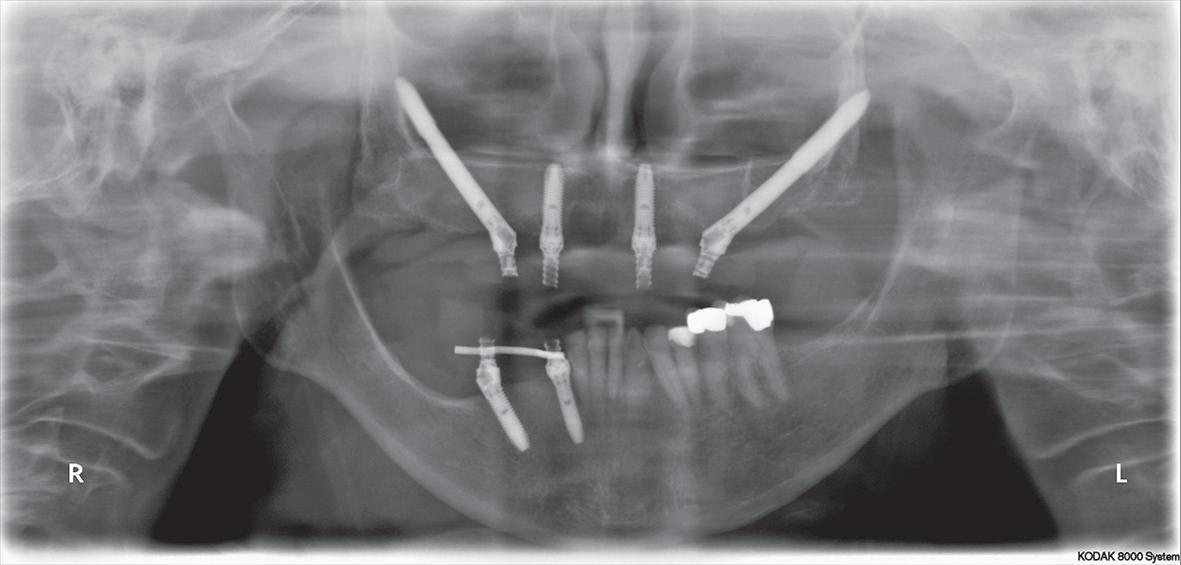
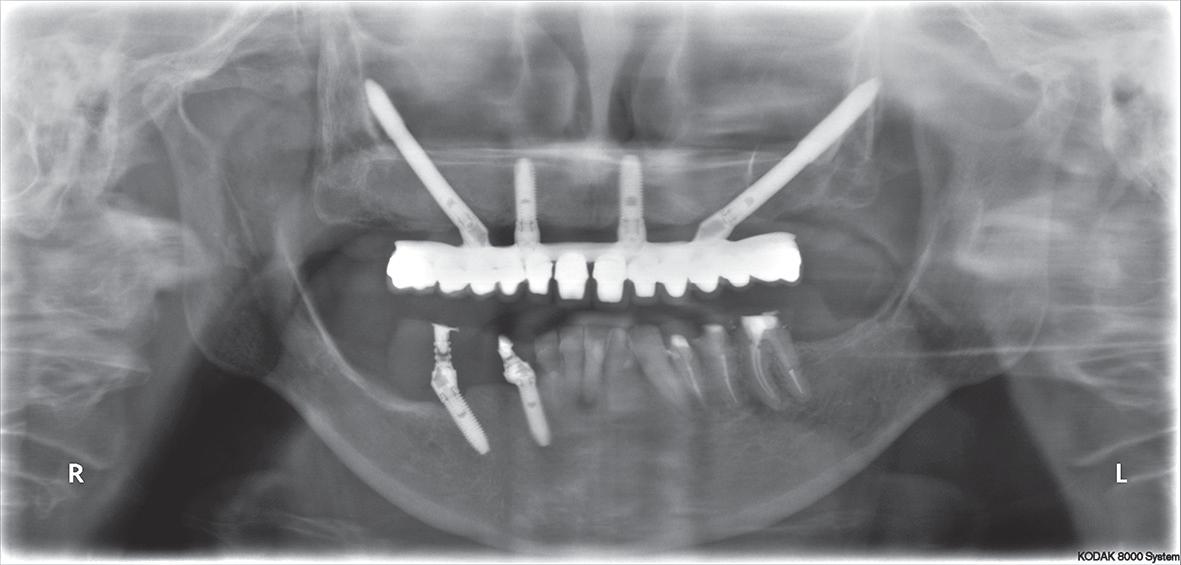
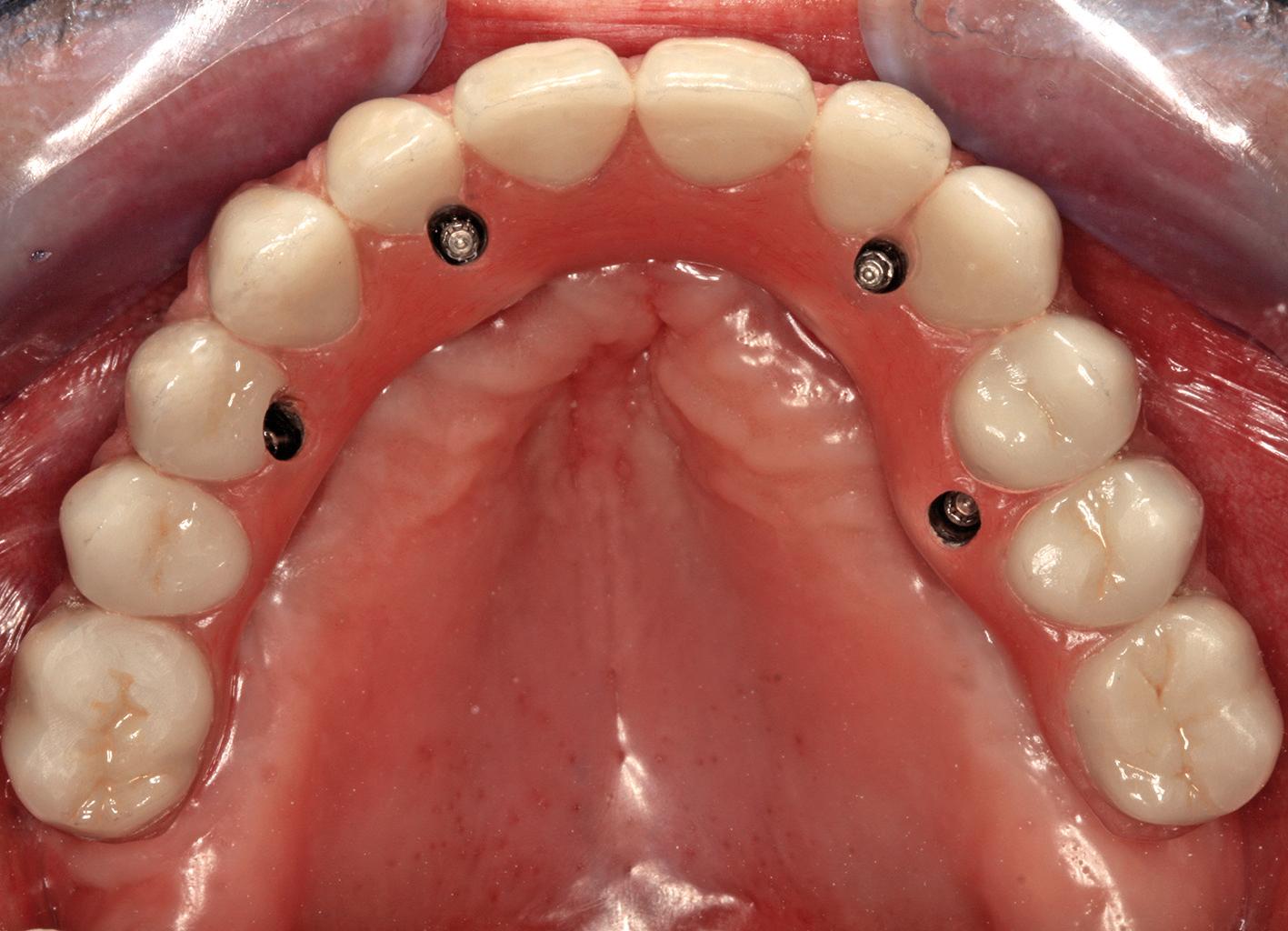
an upper and lower implant-supported fixed rehabilitation. After careful clinical and radiographic examination it was proposed to rehabilitate the upper and lower jaws according to the All-on-4 Concept (Figures 1-3). In the same surgical procedure, 2 zygomatic implants with 40 mm and 45 mm length (Nobel Biocare AB) were inserted in the posterior region and 2 standard maxillary implants (NobelSpeedy Groovy 4x13 mm RP, Nobel Biocare AB) were inserted in the anterior region of the maxilla, following the All-on-4 Hybrid (Nobel Biocare AB) protocol6. All implants achieved an insertion torque above 50N/cm which allowed immediate provisionalization (Figures 4-6). In the lower jaw, 2 implants were placed on the 4th quadrant, one distally tilted implant (NobelSpeedy Groovy RP 4x13mm, Nobel Biocare) and one axial implant (NobelSpeedy Groovy NP 3,3x13mm, Nobel Biocare)10 followed by their respective rehabilitation with screw-retained acrylic provisional crowns replacing crowns #43 to #46 (Figures 5, 6). In order to correct the occlusal plan and considering the previous extensive fillings, endodontic treatments, reinforced glass fiber posts (D.T. Light-Post Bisco Inc.; Schaumburg, USA) and provisional crowns (Heraeus Kulzer Premium Linie, Heraeus Kulzer GmbH&Co., Wasserbutg, Germany) were performed in the teeth #34 to #36. A maintenance protocol with post-operative after 2, 4 and 6 months were performed, and in the absence of signs or symptoms of peri-implant pathology, the final rehabilitation was scheduled. Taking into consideration the age, the biomechanical advantages and the patient’s aesthetic concerns, a MaloClinic Ceramic Bridge (individual Procera crowns, Zirconia copings and Nobel Rondo Zirconia Ceramic; Nobel Biocare AB) cemented onto a CAD/CAM fabricated Titanium framework (Nobel Biocare AB) with pink acrylic resin (PallaXpress Ultra, Heraeus Kulzer GmbH) was performed in the maxilla. In the mandible, a screw-retained metal-ceramic fixed partial denture was performed over the 4th quadrant implants replacing crowns #43 to #46, and individual metal-ceramic crowns were luted with GC Fuji Plus (GC, América, Inc.) to the abutments #34 to #36 (Figures 7-12). The patient was kept on a six month recall plan, and both rehabilitations remained stable through a complete follow-up period of 3 years.


Clinical implications
Due to the simplified surgical protocol associated with high success rates, the All-on-4 Concept (Nobel Biocare AB) represents a viable treatment option for the rehabilitation of the edentulous patient. The concepts principle is applicable in both partial10 and complete edentulous4-6 rehabilitations. In this particular field, the use of tilted implants in areas with high degree of bone resorption allows the connection of a fixed rehabilitation, reducing the cantilever and providing an adequate biomechanical distribution of occlusal forces. The biomechanical advantages provided by the titanium infrastructure combined with the aesthetic outcome of ceramic crowns makes the MaloClinic Ceramic Bridge as an attractive prosthetic option for the definitive prosthetic rehabilitation of complete edentulous patients10.



Correspondence
Maló Clinic: research@maloclinics.com
References
1. McDermott IG, Samant A. An overview of removable partial overdentures. Compendium 1990;11:106,108-12.
2. Fenton AH. The decade of overdentures: 1970-1980. J Prosthet Dent 1998;79:31-6.
3. Roumanas ED. The social solution-denture esthetics, phonetics and function. J Prosthodont 2009;8:112-5.
4. Maló P, Rangert B, Nobre M. All-on-4 immediate-function concept with Branemark System implants for completely edentulous maxillae: a 1-year retrospective clinical study. Clin Implant Dent Relat Res 2005;7:S88-S94.
5. Maló P, Rangert B, Nobre M. “All-on-Four” immediate-function concept with Branemark System implants for completely edentulous mandibles: a retrospective clinical study. Clin Implant Dent Relat Res 2003;5:S2-S9.
6. Malo P, Nobre M, Lopes I. A new approach to rehabilitate the severely atrophic maxilla using extramaxillary anchored implants in immediate function: a pilot study. J Prosthet Dent 2008;100:354-66.
7. Zampelis A, Rangert B, Heijl L. Tilting of splinted implants for improved prosthodontic support: a two dimensional finite element analysis. J Prosthet Dent 2007;97:35-43.
8. Krekmanov L, Kahn M, Rangert B, Lindström H. Tilting of posterior mandibular and maxillary implants for improved prosthesis support. Int J Oral Maxillofac Implants 2000;15:405-414.
9. Lan TH, Huang HL, Wu JH, Lee HE, Wang CH. Stress analysis of different angulations of implant installation: the finite element method. Kaohsiung J Med Sci 2008;24:138-43.
10. Maló P, de Araújo Nobre M. Partial rehabilitation of the posterior edentulous maxilla using axial and tilted implants in immediate function to avoid bone grafting. Compend Contin Educ Dent 2011;32:60.
11. Maló P, de Araújo Nobre M, Borges J, Almeida R. Retrievable Metal Ceramic Implant-Supported Fixed Prostheses with Milled Titanium Frameworks and All-Ceramic Crowns: Retrospective Clinical Study with up to 10 Years of Follow-up. J Prosthodont 2012. Doi:10.1111/j.1532-849X.2011.00824.x.
12. Shadid R, Sadaqa N. A comparison between screw vs. cement retained implant prostheses: a literature review. J Oral Implantol 2012 Jun;38(3):298-307.



{kind=link}